
Tags
ethics, health, healthcare, liability, malpractice, medical law, medicine, notes, study guide
Hi everyone,
I hope that you are all doing well! It’s the summer season now here and New York has been bustling. It’s nice to just eat outside and enjoy the sunny weather.
I’m finishing up the entry for my adventure blog. It’s a #tbt post so you’ll see something from the past which will have a lot of pictures. So stay tuned for that 🙂
For this handout, we go into more detail regarding medical malpractice from both the eyes of the plaintiff and of the defendant. It’s very interesting especially seeing the evolution of liability and medical care in the United States from a legal viewpoint. The condensed summary of the cases put the concepts in action. I’ve also attached articles to accompany the handout. I highly recommend reading Dr. Bal’s article “An Introduction to Medical Malpractice in the United States.” I’ve included the link from the US National Library of Medicine as well as the PDF version of it.
I finished typing this on Friday night, but will set it to publish on Saturday morning (June 11) so that it will be fresh reading for a new day. 🙂 However, if you follow the main site, the PDF and links will be posted by Friday night if you want to read it in advance.
As always happy studying and wishing you all the best,
Kevin MC
Now that we have a solid foundation of the duties and professional requirements for healthcare professionals, we will now examine the legal aspects of negligence and medical malpractice as a result of a healthcare professional failing to perform his or her duties at a standard level of care.
It is commonly known that procedures may not always go as planned and that the medical field itself is not immune to errors.
We discussed negligence and malpractice in Handout 1.3 on the section on unintentional torts. In this handout, we will go into more detail regarding the facets of negligence and malpractice as well as discuss preventative measures to avoid medical errors from occurring. Other issues that affect healthcare professionals are insurance fraud (false claims) and altering medical records.
We will examine the issues concerning both the plaintiff and defendant’s sides.
Professional Negligence and Medical Malpractice
Malpractice is defined as professional misconduct or performing one’s duties with a disregard of skill and standard level of care resulting in injury, loss, or damage to the patient. Physicians and other healthcare professionals (licensed or certified) such as nurses, technicians, mental health professionals, and pharmacists are also held to the same professional standards as physicians. The standards set by licensing and certifying bodies form the foundation of the professional level of care that is expected from healthcare professionals and their peers as they practice.
Negligence is an unintentional action resulting from an individual’s inability to perform an action that a reasonable person would have done under similar circumstances. Actions also included under negligence: individuals would perform actions contrary to the standard of care used by healthcare professionals under normal circumstances. (For example, leaving a confused patient unattended in the bathroom where he or she may slip resulting in an injury)
What constitutes as negligence or malpractice may not always be easy to determine. Cases such as a surgeon operating on the wrong area are clear, but if a medical treatment or procedure does not have the planned outcome or result (e.g. when chemotherapy is not as effective as expected), patients may take the issue to court as a result.
As we will see, medical malpractice is more complex than a patient not receiving their expected outcome. Recall from Handout 2.0 (pp. 9-10) that physicians should be clear and thorough during informed consent. One of the key points we discussed was the reasonable physician standard in which the physician should explain the details of the procedure to the best of his or her ability since it is impossible to determine any unforeseen results. So when a procedure is unsuccessful or has an unplanned result, it does not necessarily mean that malpractice has occurred.
Preventable medical errors play a role in the injury and deaths of many Americans each year. An article in the Journal of Patient Safety by Dr. John T. James estimated that 400 000 individuals were affected by preventable medical errors (preventable adverse events). (Please see the complete article in the recommended readings on the main site)
A common type of medical error is the medication error. According to the National Coordinating Council for Medication Error Reporting and Prevention (NCCMERP), a medication error is defined as “any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the health care professional, patient, or consumer…”
With medication errors, issues such as improper labeling and distribution, incorrect administration of medications, or miscommunication (e.g. misreading a prescription or lack of communication between the prescriber and the health professional administering the medication) are frequently seen in these adverse events.
The United States Food and Drug Administration (FDA) encourages individuals, healthcare professionals, and institutions to report any problems related to medical products through MedWatch, an online program to report adverse events.
Adverse events should be reported as soon as possible to ensure the patient’s safety and minimize any further risks as a result of the adverse event.
Tort of Negligence
Actions considered negligent can fall under two categories: (1) committing an act that a reasonable person would not do or (2) failing to act (inaction/omissions).
Malfeasance is defined as performing an act which is wrong and illegal. For example, when a healthcare professional who is not licensed to practice medicine (e.g. prescribe medications) or does not have the ability to request procedures to be authorized (e.g. neurological testing) does so anyway, it is considered malfeasance. This also includes giving medical advice to patients when you are not licensed to do so.
Misfeasance is defined as the improper performance of an act which is normally legal. Usually injury and damages are the result of poor techniques by the healthcare professional. Examples include if a physician unintentionally writes the incorrect dosage of a drug on a prescription (which ends up harming the patient) or when a phlebotomist injures a patient by incorrectly inserting the needle to have blood drawn. In these two cases, it’s normally legal for a physician to write prescriptions and it’s normally legal for a phlebotomist to draw blood. However, the healthcare professionals did not perform these normally legal acts properly which resulted in the injuries.
Nonfeasance is defined as failing to perform a necessary or required action. For example, if a patient is choking in a hospital and the healthcare professional present in the area does not perform the Heimlich maneuver (abdominal thrusts) to assist the patient, it is considered nonfeasance.
These are all related to the term “feasance” which means performing an act or duty.
Judgment for Negligence
In order for a court to render a judgment on a case for negligence against the defendant (the physician or other healthcare professional), the plaintiff (the patient, his or her family, guardian, or a chosen legal representative) must provide evidence that the components of the four Ds of negligence were present.
The four Ds that we will examine are
- Duty
- Dereliction (Neglect) of Duty
- Direct (Proximate) Cause
- Damages
Duty
Duty is an obligation or responsibility that each party has to each other in the physician-patient relationship. As we had discussed previously, physicians have a duty (obligation) to treat patients once a relationship has been established. Likewise, patients have a duty (obligation) to attend their scheduled appointments and follow their doctor’s instructions during treatment. If there are any issues or concerns, both parties (the physician and the patient) have a duty to notify each other. For example, during informed consent, physicians have a duty to notify patients of any adverse effects or risks that could result from medication or treatment.
In the context of mental health, mental health professionals have a duty to warn another person who may be harmed when the client/patient divulges information in private to the professional about a possibility of harming that person. If you remember from Handout 1.9 (p. 8), we discussed the case of Tarasoff v. Regents of the University of California, 17 Cal. 3d 342, 1976 in which the psychologist, Dr. Moore, failed to warn Tatiana Tarasoff when his patient Mr. Poddar discussed his threat to kill her during a private session. Mr. Poddar proceeded with the act. As a result of this case, the court decided that the safety of individuals comes before confidentiality. Thus, healthcare professionals have a duty to warn to ensure the safety and protection of individuals.
The duty of care applies the reasonable person standard. Recall that we discussed how the standard of care is expected for healthcare professionals when treating patients (i.e. when healthcare professionals use the same skill and care that a professional with the same background uses when caring for patients). The duty of care states that individuals have an obligation (duty) to act reasonably and prudently as those in similar circumstances. For example, a physician in one state is held to the same standards as a prudent and reasonable physician practicing in another state. The same applies for other healthcare professionals such as nurses, pharmacists, physical therapists, and mental health professionals.
There is also a duty of care for facilities once a patient is admitted. For example hospitals, clinics, and nursing homes have a legal duty to treat and care for a patient who has been formally admitted into the facility.
In the court setting, the judge determines duty. When the judge determines the duty of the healthcare professional, the patient has to provide evidence that he or she established a professional relationship with the physician.
Dereliction (Neglect of Duty)
Dereliction (also known as neglect) of duty is when a physician or other healthcare professional does not exercise an action accordingly that a reasonable, prudent, and ordinary peer would perform under similar circumstances. In the previous section on duty, the duty of care is founded on the reasonable person standard.
In the court setting, the patient must provide evidence that the way the physician or healthcare professional conducted procedures or treatment failed to comply with the expected standard level of care. For example, if the physician does not inform the patient that a procedure may have side effects or risks, he or she had breached the contract formed as a result of the physician-patient relationship. If the patient receives outcomes that were not discussed prior to the procedure, the physician may be charged with a dereliction of duty.
Also note that this is not the same as the patient receiving outcomes that were unanticipated or unsuccessful. As we had discussed earlier, the physician may fully inform the patient prior to the procedure that there is a chance that the results may not be successful. In this case, the physician has performed his or her duty to provide the patient with the necessary information to make an informed decision on whether to follow through with the procedure knowing that the results may not be as effective.
Direct (Proximate Cause)
Direct cause is the continuous sequence of events leading to an injury whereas the injury would not have occurred. This means that there is a cause and effect relationship–the healthcare professional’s negligence results in the patient’s injury.
Preponderance of the evidence refers to evidence presented by a party which carries greater weight (i.e. evidence that is convincing and more probable in regards to truth and accuracy) than evidence presented by the other side. The evidence shows that more likely than not the incident occurred. If the defendant presents evidence that is more convincing to the court than the plaintiff, the court will find in favor of the defendant. When both the plaintiff and the defendant present evidence that is equally convincing, the case moves in favor of the defendant. Remember from Handout 1.4 (p. 6), we discussed that the burden of proof remains on the plaintiff.
Res ipsa loquitur which is Latin for “the thing speaks for itself,” is a doctrine pertaining to negligence in which the breach of duty (negligent act) clearly caused the injury to the patient. A general guideline used by the courts to advance a case that the negligence of the physician or healthcare professional caused the patient’s injury:
- The injury would not have occurred under normal circumstances unless there was negligence involved
- The evidence shows that the cause of the injury cannot be attributed to the patient or another party (i.e. the negligence was specifically due to the defendant’s actions)
- The defendant had established a professional relationship with the patient and the negligent actions fall under the duty of the professional relationship (e.g. the physician-patient relationship)
For example, if a surgeon operates on the wrong body part or leaves an instrument inside the patient, the evidence “speaks for itself” when the plaintiff’s attorney presents the facts in court. In normal surgical circumstances, instruments cannot be left inside the patient unless the surgeon leaves it there. Since the evidence clearly points to the surgeon and the defendant had a duty to care for the patient (i.e. reasonably and prudently perform the surgical procedure to treat the patient), res ipsa loquitur can be inferred.
The defendant (the surgeon in our example) can then have a chance to disprove the presented evidence of the elements of res ipsa above.
Damages
Damages describe any financial compensation awarded to the plaintiff (the patient) due to injuries or loss caused by the defendant.
Patients can receive damage compensation for injuries related to permanent physical or mental disability, loss of earnings, costs of medical and hospital expenses, loss of enjoyment of life, and pain and suffering. When the plaintiff (the patient) receives any type of injury as a result of the defendant’s negligence, the court may award the plaintiff with compensatory damages to cover any losses or injuries from the defendant’s negligent actions.
Compensatory damages refer to the amount of money awarded by the court for the loss of income, pain and suffering, or injury suffered as a result of unlawful actions committed by another. In certain states in America, there is a cap (limit) on the amount of money awarded for negligence cases. Special (compensatory) damages are monetary awards compensating an individual who acquired financial losses as a result of an injury. For example, if the individual missed work due to the injury, he or she can be compensated for the lost earnings (if he or she had not been paid for the missed time already) or if he or she incurred additional medical expenses (such as for physical therapy or nursing care), he or she may be awarded special damages. Although the expenses were not directly caused by the defendant’s negligent actions, the individual acquired these costs because of the original negligence.
Punitive damages (also referred to as exemplary damages) are monetary awards by a court to an individual who had been harmed in a malicious and willful way. Punitive damages serve to punish the defendant committing the offense and also deter others from engaging in similar malicious conduct. For example, if an individual knowingly practices medicine without a license and severely injures a patient (e.g. an unlicensed assistant performs a procedure that paralyzes a patient), the patient can collect punitive damages. The individual deceived the patient that he or she is allowed to practice medicine and knowingly performs the procedure which could potentially harm the patient (which it did in our example). Since the actions were malicious and harmful, compensatory damages may be judged as inadequate in this case.
Nominal damages refer to small or token payments awarded to an individual by the court in which the individual had not suffered from any significant loss or injury. The amount awarded is usually small like $1 or just a few dollars to acknowledge that a patient’s legal rights were violated, but no major loss or injury had occurred.
Wrongful-death statutes are statutes established by individual states to allow the deceased’s dependents (e.g. spouse or children) or any individual responsible for handling the deceased’s assets (a court appointed administrator or named executor) to sue for wrongful death if a patient’s death was due to a physician (or other healthcare professional’s) negligence.
As we had discussed earlier, the plaintiff must provide evidence to the court to prove that the negligent actions directly caused the death of the patient (proximate cause). The plaintiff does not have to show that they were completely dependent on the deceased individual for support, but prove that there was monetary loss or injury due to the death of the individual.
Medical malpractice laws are under the jurisdiction of the individual state governments in the United States. Thus, medical malpractice cases are handled by each state government and not the federal government. (Please read the article “An Introduction to Medical Malpractice in the United States” by Dr. Bal for additional information)
Fraud
When we looked at negligence, we examined that the injuries are caused by unintentional actions. Fraud, on the other hand, is the deliberate concealment of the facts or deception by an individual for unlawful or unfair gain.
When an individual commits fraud, he or she is being dishonest in his or her actions. For example, common cases in the medical and healthcare profession are
- Insurance fraud against companies and U.S. government programs such as Medicare and Medicaid
- For example, billing for services that the physician or healthcare professional had not performed, billing for patients that don’t exist, or performing unnecessary and excessive procedures
- Another issue is when providers have personnel who are unlicensed or are told to perform duties outside of their scope of practice and the provider then bills for the services under his or her provider number
- Illegally prescribing, distributing, or selling medication (such as narcotics)
- Additional issues dealing with pharmacy fraud include billing for more expensive brand name medications, but dispensing the generic forms
- Dishonesty in medical research (e.g. falsification of data)
- Please see the case of Dr. Poisson from Handout 1.9 (p. 8) and the accompanying New York Times article
- Receiving illegal kickbacks for referrals of patients (Handout 1.3 p. 7; Handout 1.7 p. 7)
- For example, physicians may not refer patients for designated health services where they may receive illegal financial compensation (kickbacks) or may have financial interests in (e.g. referral of a patient to a medical equipment company owned by a relative or close friend)
- Workers compensation fraud and false injury claims
- Individuals may misrepresent their injury through exaggeration (e.g. continuing to stay at home even though the individual is able to work), falsely attributing an injury to a work related injury (e.g. getting injured while doing home repairs or yard work and claiming that it had occurred at the work environment)
The Office of the Inspector General (OIG) was established under the Department of Health and Human Services (HHS) to combat fraudulent activities (e.g. fraud related to false medical coding for procedures) and protect the programs under HHS such as Medicaid and Medicare.
The Office of Counsel to the Inspector General (OCIG) provides legal services such as advice and representation to the OIG. The OCIG also:
- Acts as a representative to the OIG for civil cases falling under the False Claims Act
- Imposes monetary penalties for healthcare providers who are judged guilty of fraudulent behavior
- Issues fraud alerts and offers advice on sanctions by the OIG
The False Claims Act (FCA) (31 U.S.C. §§ 3729-3733) is a federal law protecting the government from being charged for services that were
- not provided
- unnecessary
- claimed for a higher level than what was rendered (e.g. the dentist submits a claim for an X-ray when he or she just performed a routine cleaning)
- rendered using an incorrect diagnosis (e.g. the physician submits a claim for procedures under a different diagnosis instead of the patient’s real diagnosis to receive reimbursement)
- performed by an unlicensed individual
In the case of People v. Gandotra (11 Cal. App. 4th 1355 (1992), 14 Cal. Rptr. 2d 896.), Dr. Suresh Gandotra had medical assistants perform medical care in his clinic. One medical assistant prescribed and gave controlled substances to the patients and the others provided medical services. Gandotra billed the state for the unauthorized services using his provider number. The actions were caught by undercover Medi-Cal agents who posed as patients. (Medi-Cal provides affordable health coverage for eligible low income residents in the state of California) His wife Rita Gandotra was also charged for processing some of the fraudulent Medi-Cal claims. He had to pay a total of around $31000.
Healthcare professionals who violate the FCA can face civil or criminal penalties.
Major areas examined by federal statutes to combat waste, fraud, and abuse include any extra costs related to federal healthcare program (e.g. Medicaid and Medicare), quality of patient care, access to affordable and professional care, freedom for individuals to manage their care (e.g. choosing a provider and healthcare plan), competition for services, and any fraud or abuse by healthcare professionals.
We have already looked at some of these statutes such as the Stark Law and the False Claims Act. As we saw closely from these statutes, the main focus was on the financial aspects related to combatting improper referrals or illegal receipt of funds. A significant amount of money is lost every year as a result of the improper receipt of federal or state funds.
We examined in cases such as People v. Gandotra how falsifying information on claims for payments resulted in Dr. Gandotra and his wife being charged and convicted of felonies as a result of these fraudulent claims. A key thing to keep in mind is that those who are responsible for submitting these claims (such as nurses, accountants, or other office staff) should verify the accuracy of the information on the claims. Knowingly submitting fraudulent claims can result in the courts bringing civil or criminal penalties in which the defendant may be imprisoned or may have to pay large fines.
Charitable Immunity
Under common law charitable and religious organizations had immunity from civil liability. Tort immunity was given to charitable and religious organizations in the past based on the reasoning that they worked for the common good of the public.
However, this is no longer the case in modern American society. In 1942, the Appeals Court for the District of Columbia abolished charitable immunity in the case of President and Dir. of Georgetown College v. Hughes 130 F.2d 810 (D.C. Cir. 1942). From this case the court acknowledged the services that charitable organizations provide to the community and how it benefits those who do require this assistance. However, with the changing climate of charities gaining the financial resources to prevent and cover liability (i.e. be able to afford insurance), charities should be held to the same standards as private entities (e.g. individual practitioners or business corporations).
Another case reexamining charitable immunity is Abernathy v. Sisters of St. Mary’s 446 S.W.2d 599, 1969 MO in which the Supreme Court of Missouri ruled that the common law rule of charitable immunity was no longer applicable after Edward Abernathy (the plaintiff) was injured when the employee from the hospital run by the Sisters of St. Mary’s (the defendant, St. Mary’s Hospital) did not assist him when he went to use the bathroom. The employee, Marie Taylor, left him unattended in the bathroom and Mr. Abernathy sustained injuries after falling due to his current weakened condition. The court held the defendant responsible for its negligent actions.
The court stated that “immunity fosters neglect and breeds irresponsibility, while liability promotes care and caution.”
As the 20th Century progressed, society’s views changed regarding charitable organizations in which these organizations were becoming large-scale business operations with the acceptance of donations, and should be held liable for negligence if an individual gets injured as a result of that negligence. Thus, they should be able to afford and carry liability insurance to cover torts (as we had mentioned above).
Although many states (such as Missouri) and the District of Columbia abolished charitable immunity as seen from the cases above, some state jurisdictions have acknowledged forms of charitable immunity to a certain extent.
Defenses in Medical Malpractice
So far we have seen things from the plaintiff’s (e.g. patient, family, or agent) side. In this section, we will take a look at the defendant’s (e.g. physician, other healthcare professional, or facility) side where they can proceed with an affirmative defense. An affirmative defense is the set of facts introduced by the defendant to counter the claims presented by the plaintiff. In the case of medical law, the set of facts presented by the defendant aim to show evidence that the patient’s condition was the result of external factors other than the defendant’s negligence (i.e. the defendant provided a professional standard of care, but the plaintiff did not follow the aftercare instructions which resulted in the adverse event/injury). If the defendant can provide facts (to counter the prosecution’s claims) which are then proven in court, the defendant can defeat the prosecutor’s claims regarding the case.
We will now look at several other defenses:
- Denial
- Assumption of Risk
- Contributory Negligence
- Comparative Negligence
- Borrowed Servant
- Statute of Limitations
- Good Samaritan laws
- As we had examined, the burden of proof falls on the plaintiff to prove to the court that the defendant was responsible for the negligent or wrongful action. The defendant may deny the allegations and state that they are not true. This is referred to as denial. For example, if a patient sues a physician because the results of a procedure left side effects (e.g. scarring, loss of hair) or did not have a major result as anticipated, the physician can deny that he or she made any promises that the treatment would proceed perfectly. This can be documented through the informed consent forms signed by the patient in which the doctor documented that he or she stated the side effects of the procedure or that there may be a chance that the procedure may not provide the desired results/effects.
- Assumption of risk is a legal defense which prevents the plaintiff from recovering damages (either limiting or defeating his or her rights to recovery) when initiating a lawsuit since the plaintiff has full knowledge and understanding of a risk, but voluntarily decides to accept the risks of the treatment, procedure, or activity.
Smoking is a well-known example of an activity. For example, smoking is known to contribute to lung cancer in the population. If an individual continues to smoke despite the advice of healthcare professionals or other public health literature, the individual assumes the risks involved with smoking.
An example of a medical procedure with risks of complications is a craniotomy. In a craniotomy, part of the bone is removed from the skull in order to access the brain. Since the brain controls many of the body’s functions, (depending on the individual) complications from the procedure can result in infections or impairment of cognitive functions. If the physician explains these risks to the patient and the patient acknowledges their consent to treatment by signing the form, the patient assumes the risks of the complications of the procedure (on the basis that the physician maintains the expected standard level of care during the procedure).
To sum everything up, the assumption of risk defense must have these elements to be valid:
- The plaintiff (e.g. patient) must have full knowledge and understanding of the risks involved with the treatment or procedure; the physician is responsible for ensuring that the patient is fully informed of these risks regarding the proposed treatment or procedure
- The plaintiff must voluntarily choose to accept and take the risks after understanding what risks are involved
- In voluntarily choosing to accept the risks, the plaintiff must provide their consent by signing authorization forms detailing
- Contributory negligence refers to conduct on the part of the plaintiff which “contributes” to the cause of an injury. If the behavior of the plaintiff is a result of his or her negligence, he or she may receive a reduced award or even be barred from recovering financial damages from the defendant. For example, if a patient was instructed to ask for assistance if he or she needed to take a walk. If the patient decided to ignore the instructions which resulted in him or her getting injured from slipping or falling, the court can rule that the patient contributed to his or her injury since he or she did not inform the nurse or aide.
- Comparative negligence retains similar elements to contributory negligence, but examines the extent to which the plaintiff’s negligent conduct contributed to the injury. The plaintiff can recover any damages caused by the defendant’s negligence. For example, if the plaintiff was injured and the damages totaled to $20000, and the defendant was 70% responsible with the remaining 30% being the plaintiff’s fault, the plaintiff can recover $14000.
- The borrowed servant doctrine is a legal principle where an employer “borrows” an employee to temporarily work for them. The borrowed employee remains as an employee of the main employer. Under the borrowed servant doctrine, the main employer is not held accountable (not responsible) for the actions of the employee when he or she is performing services under the temporary employer.
Recall when we discussed respondeat superior in Handout 1.6 (p. 4) which discussed how the employer is responsible for the employees’ actions in the workplace setting. However, the temporary employer assumes responsibility for the borrowed employee’s actions under the borrowed servant doctrine. A well-known form of the borrowed servant doctrine is the “captain of the ship doctrine” in which a surgeon at a hospital (where the hospital is the main employer) is legally responsible for the healthcare professionals assisting in the operating room/OR (i.e. the OR nurse). Since the surgeon provides the instructions to the staff in the OR, he or she is responsible for the staff’s actions instead of the hospital. The staff is temporarily under the surgeon during the surgical procedure. In addition, the staff is also responsible for each of their individual actions during the surgery.
- The statute of limitations which we discussed in Handout 1.6 (p.3) refers to the period of time that an individual has to file a lawsuit. As we had discussed in 1.6, the individual states set the laws regarding the time limit (usually one to three years). This can protect healthcare professionals and facilities from being taken to court after a certain length of time has passed (e.g. several years after the incident had occurred). This ensures that witnesses can still be reached and allow them to recall the facts more accurately.
In addition, the statute of limitations does not take effect (“run”) until the injury is discovered. The discovery rule refers to the legal theory in which the statute of limitations begins to run when the injury is discovered. However, when fraud is involved, the statute of limitations will not begin to run until the injury is discovered.
In the case of Buchanan v. Kull (Buchanan v. Kull, 35 N.W.2d 321, Mich. 1949), the plaintiff Olive Buchanan had a thyroidectomy performed by the defendants Dr. Albert Kull and Dr. Albert Johnson. The defendants failed to exercise a professional standard of care and injured the plaintiff’s laryngeal nerves during the procedure. This paralyzed her vocal cords and she was unable to communicate with her voice. The defendants told her that her inability to vocalize was due to a lack of calcium, asthma, and a heart condition.
The plaintiff had an examination at another hospital (Ford Hospital) because she was displeased with the advice and post-operative treatment and care she had been receiving from the defendants. The examination at Ford Hospital verified the injury to the vocal cords and laryngeal nerves and this was when the injury was first discovered. As a result, the fraud exhibited by the defendants throughout her post-operative treatment (i.e. concealing the truth of the injury, giving her a fraudulent diagnosis and its associated treatment), led to the statute of limitations running when she had discovered the injury. Otherwise, the statute of limitations would have expired (the operation was performed 2 years and 2 months before she had discovered the true cause of the injury).
With respect to this case, 3 Compiled Laws of Michigan for 1929 Section 13983 regarding fraudulent concealment and discovery stated:
“Where a cause of action is fraudulently concealed from a person entitled thereto, such person may commence an action within 2 years after he discovers it although it would be otherwise barred by the statute of limitations”
“Fraudulent concealment, tolling statute of limitations, means employment of artifice, planned to prevent inquiry or escape investigation, and mislead or hinder acquirement of information disclosing a right of action and acts relied on must be of an affirmative character and fraudulent”
As we had seen from the case, the defendants had full knowledge that their negligent actions caused the injury and attempted to conceal it from the plaintiff. Although time had passed, fraud had occurred in the concealment of the true nature of the injury. This allowed the plaintiff to pursue litigation upon the discovery of the injury from the examination at Ford Hospital.
- We discussed the Good Samaritan Laws in greater depth in Handout 1.6 (p. 4). Good Samaritan laws protect off-duty healthcare professionals and lay citizens who are assisting individuals during emergencies.
Remember that healthcare professionals are not protected by Good Samaritan laws if they are performing actions and services in their place of employment.
Res Judicata
Res judicata which is Latin for “the thing has been decided,” refers to cases in which (1) a final judgment has been issued between the plaintiff and the defendant and (2) the appeals process is over, and thus, the plaintiff may not be able to carry out a new lawsuit on the same matter against the same defendant.
For example, a patient sues a physician and hospital as a result of a severe allergic reaction after being administered penicillin when it was established that he or she was allergic to it. After both sides presented their cases in court, the judge ruled in favor of the patient. The patient cannot initiate a new lawsuit against the same hospital and physician for the same set of facts (i.e. the penicillin error) from the incident.
You can download the PDF version of this Handout Here
My complete Mathsci Review Site











 ≈0.67
≈0.67



 or
or 
 = 21 ÷ 3 = 7
= 21 ÷ 3 = 7
 and we know that a proper fraction has to combine with the whole number.
and we know that a proper fraction has to combine with the whole number.

 into a mixed number.
into a mixed number.



























 and
and  .
.

 ×
×
































































 . So if we turn our proportion into fraction form:
. So if we turn our proportion into fraction form:



























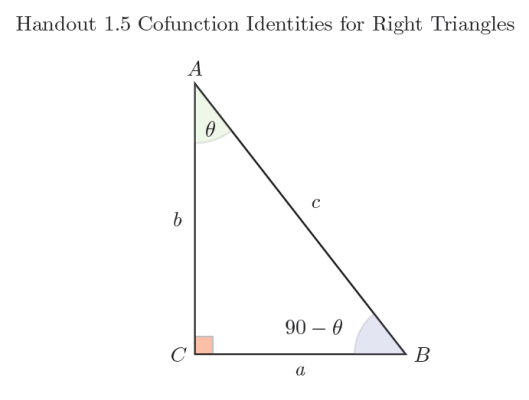
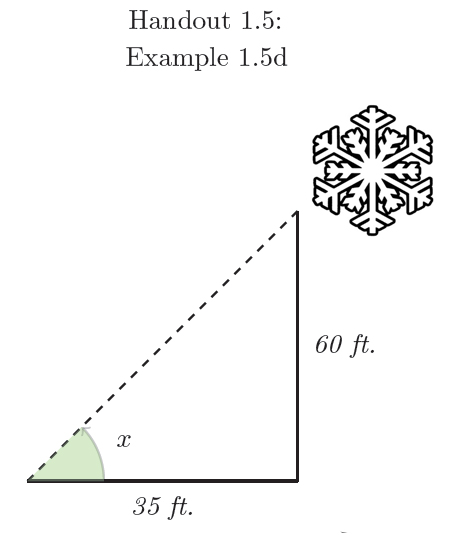
 with 90˚ since we learned that
with 90˚ since we learned that 
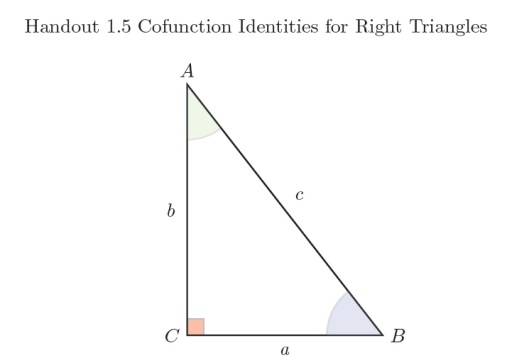
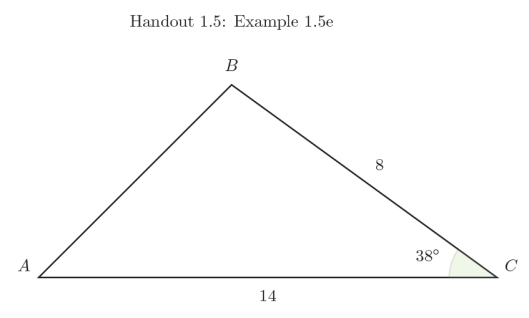
 which can now be applied to our triangle.
which can now be applied to our triangle.












 ) since it is given in radians instead of degrees.
) since it is given in radians instead of degrees.

 ≈ 2.6131
≈ 2.6131
 , we learned that θ = 45˚ or
, we learned that θ = 45˚ or  in the 45-45-90 isosceles triangle since according to our right triangle definitions, sin θ =
in the 45-45-90 isosceles triangle since according to our right triangle definitions, sin θ =  .
. , we learned that θ = 60˚ or
, we learned that θ = 60˚ or  in the 30-60-90 triangle since according to our right triangle definitions, tan θ =
in the 30-60-90 triangle since according to our right triangle definitions, tan θ =  .
.




 .
.







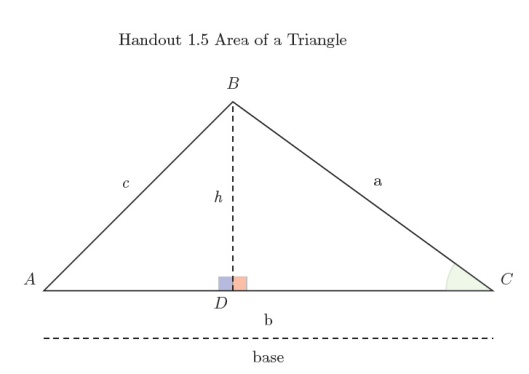







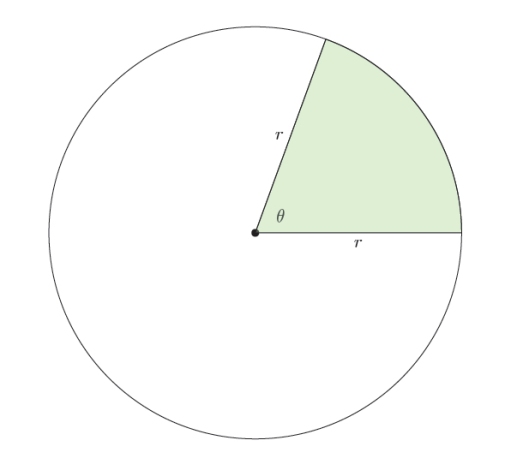
 of the entire pizza pie). Similarly, the shaded region is what we focus on.
of the entire pizza pie). Similarly, the shaded region is what we focus on. or
or  . Since the area of a complete circle is A = 𝝅r2, we include the area of a sector as a part of the complete circle and then express it as:
. Since the area of a complete circle is A = 𝝅r2, we include the area of a sector as a part of the complete circle and then express it as:
 and cancel out the 𝝅 as we multiply and simplify:
and cancel out the 𝝅 as we multiply and simplify:













 and x for
and x for 


![=\frac{12(sin\hspace{1mm}6\theta)+\hspace{1mm}2(sin\hspace{1mm}5\theta)}{3[(sin\hspace{1mm}5\theta)(sin\hspace{1mm}6\theta)]}](https://s0.wp.com/latex.php?latex=%3D%5Cfrac%7B12%28sin%5Chspace%7B1mm%7D6%5Ctheta%29%2B%5Chspace%7B1mm%7D2%28sin%5Chspace%7B1mm%7D5%5Ctheta%29%7D%7B3%5B%28sin%5Chspace%7B1mm%7D5%5Ctheta%29%28sin%5Chspace%7B1mm%7D6%5Ctheta%29%5D%7D&bg=ffffff&fg=000&s=1&c=20201002)








 =
= 

 ≠ -1
≠ -1




![\frac{d}{dx}[\frac{1}{3}x^3+2x^2+2x+C]](https://s0.wp.com/latex.php?latex=%5Cfrac%7Bd%7D%7Bdx%7D%5B%5Cfrac%7B1%7D%7B3%7Dx%5E3%2B2x%5E2%2B2x%2BC%5D&bg=ffffff&fg=000&s=1&c=20201002)
![= \frac{1}{3}\frac{d}{dx}[x^3]+2\frac{d}{dx}[x^2]+2\frac{d}{dx}[x]+\frac{d}{dx}[C]](https://s0.wp.com/latex.php?latex=%3D+%5Cfrac%7B1%7D%7B3%7D%5Cfrac%7Bd%7D%7Bdx%7D%5Bx%5E3%5D%2B2%5Cfrac%7Bd%7D%7Bdx%7D%5Bx%5E2%5D%2B2%5Cfrac%7Bd%7D%7Bdx%7D%5Bx%5D%2B%5Cfrac%7Bd%7D%7Bdx%7D%5BC%5D&bg=ffffff&fg=000&s=1&c=20201002)








![\frac{d}{dx}[-csc\hspace{0.8mm}x+C]](https://s0.wp.com/latex.php?latex=%5Cfrac%7Bd%7D%7Bdx%7D%5B-csc%5Chspace%7B0.8mm%7Dx%2BC%5D&bg=ffffff&fg=000&s=1&c=20201002)
![=(-1)\frac{d}{dx}[csc\hspace{1mm}x]+\frac{d}{dx}[C]](https://s0.wp.com/latex.php?latex=%3D%28-1%29%5Cfrac%7Bd%7D%7Bdx%7D%5Bcsc%5Chspace%7B1mm%7Dx%5D%2B%5Cfrac%7Bd%7D%7Bdx%7D%5BC%5D&bg=ffffff&fg=000&s=1&c=20201002)







 , just find the derivative of the function.
, just find the derivative of the function.


 .
. with each solution having different constants. Since it is the constants that differ for the antiderivatives of f(x), we can observe that each antiderivative is a vertical translation of each other.
with each solution having different constants. Since it is the constants that differ for the antiderivatives of f(x), we can observe that each antiderivative is a vertical translation of each other. and observe a few of its solutions. A few values of C included here are 2.5, -2.5, 5, and -5.
and observe a few of its solutions. A few values of C included here are 2.5, -2.5, 5, and -5.
 .
.












 . If you want to factor it out you can write it as
. If you want to factor it out you can write it as  .
. (unlike in our previous example where we began with
(unlike in our previous example where we began with  ).
).

 and solve for C.
and solve for C.
 .
. .
.

 and solve for C.
and solve for C.

 .
. or
or  . By integrating
. By integrating  .
. .
.

 .
.
 . We now integrate the velocity function to get the position function s(t).
. We now integrate the velocity function to get the position function s(t).








